Table of Contents >> Show >> Hide
- What Is Cubital Tunnel Syndrome?
- Cubital Tunnel Syndrome Symptoms
- What Causes Cubital Tunnel Syndrome?
- Who Is More Likely to Develop It?
- How Doctors Diagnose Cubital Tunnel Syndrome
- Cubital Tunnel Syndrome Treatment Options
- Types of Cubital Tunnel Syndrome Surgery
- Recovery and Outlook
- Can You Prevent Cubital Tunnel Syndrome?
- When to See a Doctor
- What Real-Life Experiences With Cubital Tunnel Syndrome Often Look Like
- Conclusion
If your ring finger and pinky keep going numb every time you hold your phone, drive for a while, or sleep like a human pretzel, your elbow may be trying to send you a strongly worded complaint. One possible reason is cubital tunnel syndrome, a condition caused by irritation or compression of the ulnar nerve at the inside of the elbow. It can start out as a mild annoyance and gradually turn into weakness, clumsiness, and pain that makes everyday tasks feel unnecessarily dramatic.
The good news is that cubital tunnel syndrome is treatable. Many cases improve with simple changes like avoiding pressure on the elbow, using a nighttime splint, and adjusting daily habits. More stubborn or severe cases may need medical treatment or surgery. In this guide, we will break down the symptoms of cubital tunnel syndrome, what causes it, how it is diagnosed, and the most common cubital tunnel syndrome treatment options available today.
What Is Cubital Tunnel Syndrome?
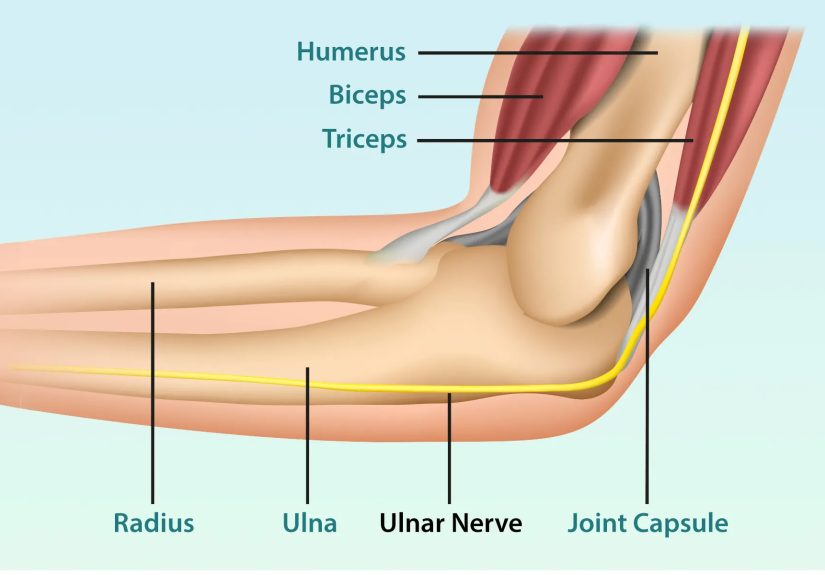
Cubital tunnel syndrome happens when the ulnar nerve gets compressed, stretched, or irritated as it passes through the cubital tunnel, a narrow space on the inside of your elbow. The ulnar nerve is the same nerve involved when you hit your “funny bone,” except there is nothing especially funny about repeated tingling, weakness, or hand pain.
This nerve helps provide sensation to the little finger and part of the ring finger. It also controls several of the small muscles in the hand that support grip strength, finger coordination, and fine motor skills. When the nerve is under too much pressure, the messages traveling along it become disrupted. That is when symptoms begin to show up.
Compared with carpal tunnel syndrome, which affects the median nerve at the wrist, cubital tunnel syndrome affects the elbow side of the arm and usually produces symptoms on the small-finger side of the hand. Different tunnel, different nerve, equally annoying.
Cubital Tunnel Syndrome Symptoms
Cubital tunnel syndrome symptoms often start gradually. At first, the signs may come and go. Over time, they can become more persistent, especially if the nerve keeps getting irritated.
Common early symptoms
- Numbness and tingling in the ring finger and pinky
- Symptoms that get worse when the elbow is bent
- Tingling or pain that wakes you up at night
- Aching pain on the inside of the elbow
- A strange electric or burning sensation that travels into the forearm or hand
More advanced symptoms
- Weak grip strength
- Hand clumsiness or dropping objects
- Difficulty typing, buttoning clothes, or spreading fingers apart
- Weakness in pinch strength, especially when holding keys, paper, or utensils
- Visible muscle loss in the hand in severe or long-standing cases
A classic clue is that symptoms flare when the elbow stays bent for a long time. That can happen while talking on the phone, sleeping with an arm tucked in, reading in bed, or driving with a bent elbow resting on the door. In other words, normal life has many surprisingly effective ways to annoy the ulnar nerve.
What Causes Cubital Tunnel Syndrome?
In many people, there is not one dramatic cause. Instead, the nerve gets irritated by repeated stress, pressure, or stretching over time. The cubital tunnel is a tight space to begin with, and bending the elbow can increase pressure on the nerve.
Common cubital tunnel syndrome causes
- Frequent elbow bending, especially for long periods
- Leaning on the elbow on hard surfaces
- Sleeping with the elbow bent
- Direct injury to the inside of the elbow
- Bone spurs, arthritis, fractures, or dislocations around the elbow
- Swelling or inflammation that narrows the tunnel
- Anatomical differences that make the nerve more likely to rub or shift
Some people also have a nerve that moves or “snaps” over the bony part of the elbow during motion. Others develop symptoms because of repetitive work or sports that keep the elbow flexed again and again. Desk work, driving, machine operation, weight training, and some throwing or lifting activities can all contribute in certain cases.
It is also worth noting that the cause is sometimes unknown. So if you are trying to solve the mystery by replaying every elbow-related event of the past five years, your nerve may refuse to provide a clear confession.
Who Is More Likely to Develop It?
Anyone can develop cubital tunnel syndrome, but the risk may be higher in people who:
- Spend long hours at a desk with elbows bent
- Rest elbows on hard armrests or table edges
- Sleep with arms tucked in tightly
- Do repetitive work involving bending, pulling, lifting, or reaching
- Have had a previous elbow injury
- Have elbow arthritis or structural changes around the joint
Some people notice symptoms only during certain activities, while others feel them almost all the time. The difference often depends on how irritated the nerve is and how long the compression has been going on.
How Doctors Diagnose Cubital Tunnel Syndrome
A diagnosis usually starts with your symptoms, your daily habits, and a physical exam. A clinician may ask when the numbness happens, whether it wakes you at night, and whether you feel weakness or clumsiness in the hand.
Physical exam
During the exam, a provider may check:
- Areas of numbness in the ring and little fingers
- Hand strength and finger coordination
- Whether bending the elbow reproduces symptoms
- Whether tapping over the nerve causes tingling
- Whether the nerve seems unstable or slips over the elbow bone
Tests that may be used
- Nerve conduction studies to see how well signals move through the ulnar nerve
- Electromyography (EMG) to evaluate nerve and muscle function
- X-rays to look for arthritis, bone spurs, or old injuries
- Ultrasound to assess the nerve and nearby structures
- MRI in selected cases if another problem is suspected
Testing is not always necessary in mild, very typical cases, but it can be helpful when the diagnosis is unclear, symptoms are more severe, or surgery is being considered. It can also help rule out other problems, such as a pinched nerve in the neck or a different nerve compression elsewhere in the arm.
Cubital Tunnel Syndrome Treatment Options
Cubital tunnel syndrome treatment depends on how severe the symptoms are, how long they have been going on, and whether weakness or muscle changes are already present. In many mild to moderate cases, nonsurgical treatment is tried first.
Nonsurgical treatment
Conservative care aims to reduce irritation, limit prolonged elbow flexion, and protect the ulnar nerve from repeated pressure.
- Activity modification: Avoid leaning on the elbow and reduce repetitive bending when possible.
- Night splinting or bracing: Keeping the elbow straighter during sleep can reduce nerve tension.
- Elbow padding: A padded sleeve or elbow pad can protect the nerve from hard surfaces.
- Rest: Giving the irritated nerve a break from aggravating activities may calm symptoms down.
- Anti-inflammatory medicine: Some people use medications recommended by their clinician for pain or inflammation.
- Hand or occupational therapy: Therapy may include education, stretching, and nerve gliding exercises in selected cases.
These measures are often most effective when symptoms are still mild and muscle weakness has not become significant. The earlier the nerve irritation is addressed, the better the chances of improvement without surgery.
When surgery may be needed
Surgery may be recommended when:
- Nonsurgical treatment does not relieve symptoms
- Numbness becomes persistent rather than occasional
- There is noticeable hand weakness
- Muscle wasting appears
- Tests show more severe nerve compression
This is important because long-standing nerve compression can become harder to reverse. If a hand is already getting weaker or smaller, that is not the moment to keep negotiating with your elbow like it is a moody roommate.
Types of Cubital Tunnel Syndrome Surgery
There is not just one surgical approach. The best option depends on the anatomy of the elbow, the severity of the compression, whether the nerve is unstable, and the surgeon’s judgment.
1. In situ decompression or cubital tunnel release
This procedure releases the tissue that is compressing the nerve without moving the nerve from its usual location. It is commonly performed and may work well in many patients.
2. Ulnar nerve transposition
In this procedure, the nerve is moved to a new position in front of the elbow bone so it is under less stretch or pressure during motion. This may be chosen if the nerve is unstable or snaps over the bone.
3. Medial epicondylectomy
In selected cases, a portion of the bony prominence on the inside of the elbow is addressed to reduce pressure on the nerve. This is less commonly discussed by patients but is part of the surgical toolbox.
Many cubital tunnel surgeries are outpatient procedures, meaning you go home the same day. Recovery varies. Some people feel better fairly quickly, while nerve recovery in more severe cases can take much longer. If symptoms have been present for a long time, surgery may stop further worsening more reliably than it reverses every symptom completely.
Recovery and Outlook
The outlook depends on how irritated the nerve is and how early treatment begins. Mild cases may improve with habit changes and splinting. More advanced cases can still improve, but recovery may be slower, especially if weakness or muscle loss was already present before treatment started.
After surgery, soreness at the elbow is common at first. Movement usually returns gradually, and some people also do hand therapy as part of recovery. Sensory symptoms may improve before strength fully returns, and persistent long-term compression may leave some lingering deficits.
That sounds ominous, but it is really just a reminder not to ignore symptoms for months while hoping your ring finger will suddenly become less offended by your sleeping position.
Can You Prevent Cubital Tunnel Syndrome?
You cannot prevent every case, but you can lower the odds of irritating the ulnar nerve.
- Avoid resting your elbow on hard surfaces for long periods
- Use a headset instead of holding the phone with your elbow bent
- Adjust desk height and arm support for better ergonomics
- Take breaks during repetitive work or training
- Sleep with the arm in a more neutral position if possible
- Warm up before sports or repetitive upper-extremity activity
Small changes can make a surprisingly big difference. Sometimes prevention is not glamorous. It is just a pillow, a pad, a better chair, and fewer heroic attempts to answer emails with your elbow folded like a pocketknife.
When to See a Doctor
You should seek medical evaluation if you have:
- Numbness or tingling that keeps coming back
- Symptoms that worsen when the elbow is bent
- Nighttime symptoms that interfere with sleep
- Weak grip or hand clumsiness
- Visible muscle wasting in the hand
- Pain or symptoms that are affecting work, exercise, or daily activities
Because cubital tunnel syndrome can overlap with other conditions, a proper evaluation matters. Not every tingling finger is an elbow issue, and not every elbow issue should be handled with internet optimism and a random compression sleeve.
What Real-Life Experiences With Cubital Tunnel Syndrome Often Look Like
Many people do not realize they may have cubital tunnel syndrome at first because the earliest signs can feel random. Someone might notice that the pinky and ring finger go numb during a commute, then return to normal later. A side sleeper may wake up at 3 a.m. shaking their hand, assuming they just slept wrong. A desk worker may blame the keyboard, the mouse, the chair, Mercury in retrograde, or all of the above before anyone looks closely at the elbow.
A common experience is that symptoms become more obvious during quiet activities rather than heavy exercise. Holding a phone, reading on a couch, driving, or resting the elbow on an armrest can trigger tingling surprisingly fast. Some people describe it as a buzzing sensation. Others say it feels like a dull, creeping numbness that starts in the elbow and slides into the hand. Once symptoms become frequent, many notice weakness too. Coffee cups feel less secure. Keys are harder to pinch. Typing can feel slightly off. Opening jars becomes a team sport.
People with more advanced compression often say the most frustrating part is not the pain, but the clumsiness. The hand simply does not feel reliable. Buttons, zippers, phone grips, and utensils suddenly demand more concentration than they should. Athletes may feel a subtle drop in control during lifting, throwing, or gripping. Musicians may notice finger coordination problems before anything else. For workers who use tools all day, symptoms can become both uncomfortable and expensive.
Nighttime is another recurring theme in patient experiences. Many people sleep with their elbows tightly bent without realizing it, and they wake with numb fingers or a burning ache along the inner forearm. Once they start using a nighttime brace or even a soft towel wrap to limit deep elbow bending, they often notice meaningful relief. It is not glamorous. No one feels especially stylish sleeping like they are protecting a baguette under the blanket. But it can help.
Those who improve with conservative treatment often say the turning point was not one dramatic intervention. It was a stack of small changes: better posture, fewer hard armrests, more breaks, less elbow bending, smarter sleep positioning, and finally paying attention to what triggers symptoms. On the other hand, people who delay care sometimes realize only later that persistent numbness and weakness were signs the nerve needed more serious attention.
For people who end up needing surgery, the emotional experience is often a mix of relief and impatience. Relief because there is finally a plan. Impatience because nerves do not recover on the same schedule as a scraped knee or a bruised ego. Improvement can be gradual. Many patients feel better knowing that early treatment generally offers a better chance of recovery, while long-standing severe compression may take longer and may not fully reverse. That reality can sound discouraging, but it is also empowering. The sooner symptoms are recognized, the better the odds of protecting hand function and getting back to normal life with fewer tingles, fewer dropped objects, and a lot less elbow drama.
Conclusion
Cubital tunnel syndrome is one of the most common nerve compression problems affecting the arm, and it can range from mildly irritating to seriously disruptive. The hallmark signs are numbness and tingling in the ring and little fingers, especially when the elbow is bent, along with inner elbow pain, weak grip, and hand clumsiness in more advanced cases.
The condition is often caused by repeated elbow bending, leaning on the elbow, sleeping with the arm bent, or structural problems around the joint. Fortunately, many people improve with nonsurgical treatment such as activity changes, nighttime splinting, elbow padding, and therapy. When symptoms persist or weakness appears, surgery may be the next step to relieve pressure on the nerve and prevent further damage.
The biggest takeaway is simple: do not ignore recurring numbness in your pinky and ring finger. Your elbow may be delivering a very real message, and it is better to read it early than wait for the sequel.





